Published 25 July 2022
FINDING THE ENGAGEMENT SWEET SPOT OF MEDICAL COMMUNICATIONS
There are two main challenges for healthcare communications today: 1) getting content in front of healthcare professionals (HCPs) and 2) ensuring that they engage with the content. The focus of this commentary is the second challenge – once HCPs have seen a piece of content, how can we ensure that they will truly engage with it?
And what do I mean by engage? I’m not speaking of an HCP merely seeing some content.
According to the Oxford English dictionary, to be engaging, the content must “succeed in attracting and keeping somebody’s attention and interest.” The Moore’s Levels for assessing the impact of continuing medical education go all the way from Level One ‘participation’ (traffic, basically) to Level Seven ‘community health’, something that is quite hard to measure, let alone link directly to a piece of content. So, for the sake of simplicity, I will use Oxford’s definition for engage.
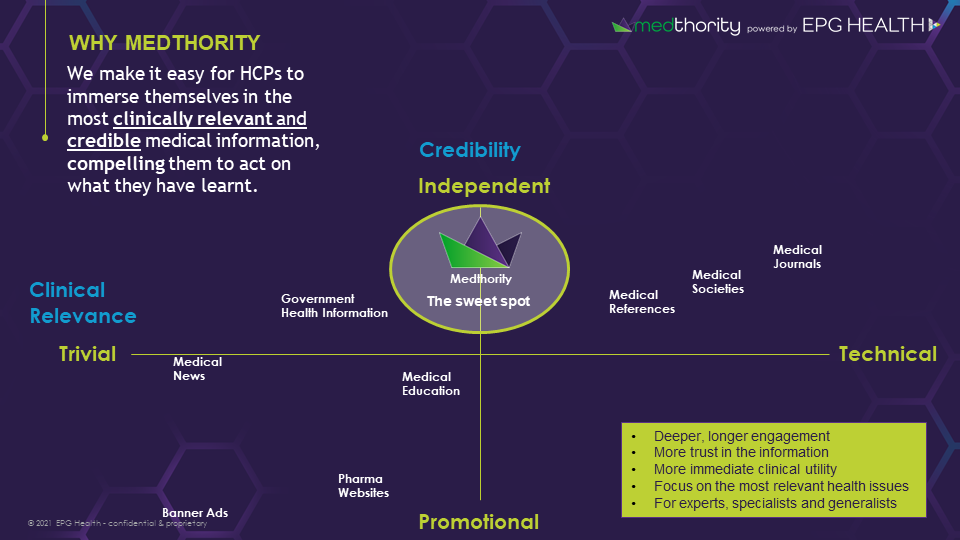
Critical success factors then for engaging content are relevance to HCPs’ clinical practice, credibility to their above-average intelligence, and compelling enough to instil a change in their behaviour.
Considering these criteria for engaging content, here are some examples of recent medical communications I and my team have come across on various HCP platforms. How do they measure up to these success factors for ‘engaging’ content?
1. Single-cell transcriptomics of lupus nephritis with ANCA positive
2. Effect of Robot-Assisted Radical Cystectomy With Intracorporeal Urinary Diversion vs Open Radical Cystectomy on 90-Day Morbidity and Mortality Among Patients With Bladder Cancer: A Randomized Clinical Trial
3. Doctor hires hitman to kill ex-husband
4. Different questions. Same Answer…The only protease inhibitor-free, pangenotypic, panfibrotic HCV regimen
5. Third Person ‘Cured’ of HIV via Transplant
6. Pneumonia is an infection of the lungs that can cause mild to severe illness in people of all ages…[or is it]…Pneumonia is swelling (inflammation) of the tissue in one or both lungs.
7. 2 reasons to prescribe the #1 branded long-acting injectable antipsychotic for schizophrenia or schizoaffective disorder…( I stopped watching the banner animation at this point, never making it to the actual brand name)
Not one of these examples really hits the sweet spot of clinical relevance and credibility to maximise engagement with HCPs, and therefore, not one is likely to be capable of compelling HCPs to adapt their behaviour in order to better serve their patients.
Regarding clinical relevance, some are too trivial, bearing no relation to HCPs’ day to day clinical practice. Triviality could veer into clickbait territory, or it could simply be too early, too experimental, and not something that is likely ever to impact their clinical practice. Others are certainly not trivial, having substantial potential to improve patient care, but are written in a way that is inaccessible to all save the top experts in a field. The sweet spot of clinical relevance aims to find the balance between triviality and technicality, maximising both the level of detail and immediate applicability of the medical information being conveyed.
Regarding credibility, some of these communications would turn off most HCPs, simply by their outlandish claims. Flat out promotional advertising, while perhaps suitable for consumer goods, really has no place in healthcare communications. As Roche Pharmaceuticals’ former CEO William Burns put it best over a decade ago, such advertising “was the single worst decision for the industry. When industry says we’re spending all the money on R&D but actually it’s spending it on TV advertising to preserve margins, it doesn’t get much credibility.” I would apply the same logic to banner advertising, and a good number of other pharma-led digital initiatives, 96% of which fail, according to Fierce Pharma ’s reporting on research by Graphite.
However, fully independent information, without the expert input and even proper commercial incentives of pharma, can also be misleading, as exemplified by the competing definitions of pneumonia by the CDC and NHS, respectively, in example 6. The sweet spot of credibility must then necessarily involve pharma, but must retain sufficient independence to remain credible.
The final factor in engagement is compelling HCPs to change their behaviour. One potential way to spur HCPs to action is to expose gaps between their medical knowledge or practice and patient perspectives. Working with patient experts or advocates is an excellent way to create useful conversations between patients and HCPs, often to the mutual benefit of both. We have recently launched patient-doctor discussions in podcasts, leaflets for HCPs to use with patients, and infographics highlighting issues surrounding patient quality of life. Despite the patient focus, we are seeing strong engagement with this content that is intended only for HCPs.
At EPG Health, we are seeking to find this sweet spot for everything we publish on Medthority (www.medthority.com) and I believe we are on the right track as demonstrated by the engagement metrics we are seeing in our disease area-specific Learning Zones.
• 1 in 3 Medthority visits are to Learning Zones (client-funded) versus other content (news, drugs, journals, guidelines and clinical trials)
• 6.7 page views per session on average per Learning Zone
• 7:18 minutes average session duration
• 90% of HCPs confirm Learning Zones support their clinical decisions
• 59% of visitors return
When pharma and independent medical education platforms, like Medthority, collaborate effectively to engage HCPs with the most clinically relevant and credible medical information, compelling them to act on what they have learned, perhaps we will see attributable improvements in community health, finally achieving Moore’s Level Seven.
To learn more about how EPG Health aims to hit the engagement sweet spot, please see ‘Our Approach’ or book a meeting so we can discuss.
About the author
HEAD OF SCIENTIFIC SERVICES
Ben leads our team of science writers based in the UK, France & Australia. Ben has PhD in Biology (Neuroscience), BS in Molecular Biology, University of California, San Diego. 8 years producing compliant digital healthcare content. R&D, clinical and research, including 3-year postdoc.
News & Views
MORE ARTICLES